Communication about pain
Communication about pain (CRT)
Cognitive Rehabilitation Therapy – Communicating about pain.
Communication about pain is communication about feelings. However, it is a big challenge for the therapist to explain this to patient, and especially for the tissue/structure oriented patient, easily feeling stigmatized. ”What! Are you telling me that the pain I am experiencing is in my head? No, my pain is in my muscle, my tendon, my ligament, my intervertebral disc, etc. I am not a psycho!”
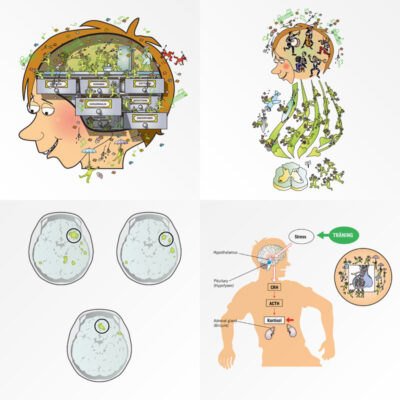
Using pictures and text with a humorous tone is a new way to avoid the problem of patients feeling stigmatized. When the patient recognizes him/herself in the pictures the patient often start to talk about what the picture means to him/her. Now the therapist can guide and add information in relation to what the patient is telling. Guiding insted of explaining, is a biopsychosocial way of incerasing the patients knowledge about the patients pain.
Cognitive Rehabilitation Therapy (CRT) is founded in and based on explanatory models of pain psychology and pain physiology combined with physical activity to modulate pain. These explanatory models are adapted and applied practically through exposure and graded exercise terapy that is integrated in Medical Exercise Therapy (MET).
The aim of CRT is to increase a patient’s knowledge and allow them to gain better control of their symptoms. CRT is a form of exposure therapy where the main goal is to decrease fear, decreasing different psychological reactions to pain. Furthermore, CRT aims to improve a patient’s functional level and increase confidence in their own abilities.
Why CRT and not CBT (Cognitive behavioral therapy)? CBT is a clearly defined and evidenced based method for certain behavioral conditions that is generally applied by a psychologist. To avoid confusion, I call the method presented Cognitive Rehabilitation Therapy which incorporates certain components of CBT like exposure.
 Most agree on this: Our treatment methods relieve pain. However, the treatment technique is not the most important key to pain relief. Research has shown and taught us something interesting. Paradoxically, merely increasing ones knowledge about pain reduces pain. Thoughts and feelings can increase or decrease nociceptive input to and in the central nervous system. Simply put, the patient’s own thoughts and feelings can either increase or decrease pain. Importantly, it is the patients understanding and own explanations together in communication with the therapist that are very important factors in treatment – possibly the most important. Communication relieves pain.
Most agree on this: Our treatment methods relieve pain. However, the treatment technique is not the most important key to pain relief. Research has shown and taught us something interesting. Paradoxically, merely increasing ones knowledge about pain reduces pain. Thoughts and feelings can increase or decrease nociceptive input to and in the central nervous system. Simply put, the patient’s own thoughts and feelings can either increase or decrease pain. Importantly, it is the patients understanding and own explanations together in communication with the therapist that are very important factors in treatment – possibly the most important. Communication relieves pain.
We have no pain receptors, only nociceptors.
The health and medical world is in the midst of a big challenge. The normal and pre-existing understanding for what pain is must change. We must take on a new model of pain and communicate this to our patients. That an acute tissue injury like spraining the ankle, causes pain is no big surprise for anyone. However, it is more difficult to understand why it continues to hurt 8-12 weeks later, when the swelling has subsided and all the tissues (ligaments, tendons) in the ankle have theoretically healed. Now the pain experience do not sit primarily in the tissues, but rather is a result of changes in the nervous system. More related to different feelings, or more specifically an experience, that is first processed and further produced by different areas of the brain.
Under x-ray, MR -, and ultrasound scanning we can see various soft tissues. When we see a change or degeneration in one or more tissues we might be quick to think that here is the reason for the pain. This is erroneous. The continuum between seeing tissue changes on x-ray, MR-, and ultrasound scanning pain and function is very long and there often exists no connection. The reason for this is that we don’t have any pain receptors. This knowledge has existed over more than 40 years. Instead, the body has high tolerance nociceptors for sensing mechanical load, heat, cold and chemical reactions, that might be dangerous for us. Unfortunately, over a long time we have wrongly associated nerve impulses from nociceptors as pain signals.
A tissue injury or a sprained ankle for example, reduces the firing threshold for various nociceptors. They send nerve impulses to the spinal cord and further on to various areas of the brain. If the brain interprets the situation as dangerous (or threat value for your survival) you will experience pain. Thus, pain is an OUTPUT and not an INPUT. The pain you feel is also context related. Meaning that a tissue injury to a finger feels much more painful or dangerous for a professional violin player who is dependent on fine coordinative movements of his fingers to play his instrument compared to a person that has a type of occupation where this function is not that important. This knowledge about pain gives us a great opportunity to treat pain. We get a better understanding on how it is possible to have a prolapse of an intervertebral disc in the back, knee osteoarthritis or other structural changes and still be symptom free. When you realize that pain is closely related to feelings, an interpretation, it becomes easier to understand how close psychological factors can affect discomfort and pain.
Communication is difficult
Communication is also complicated. When explaining something to your patient, the patient will forget 25 percent of what you explained straightaway. Out on the street are a further 25 percent forgotten. The last 50% the patient interpret depending on beliefs, feelings, mood and day. You want your message and concepts to be understood. It is decisive that you get the patient to “mirror” your information and concepts.
Holten Institute har created efficient tools for the mirroring process


Three posters about pain
The Holten Institute has developed effective tools for the mirroring process.
-3 posters (with accompanying animations)
-4 illustrations that mirror various aspects of pain
-And the book: The Mirror Book
In our on-line shop you can purchase the posters, illustrations, the animations and the Mirror Book.